BOX ADS HERE
Zika virus is a mosquito-transmitted infection that has ravaged most of Latin America, the Caribbean and now Europe. Here are some answers and advice about the outbreak you need to know.

Zika virus is a mosquito-transmitted infection
The World Health Organization has declared the Zika virus an international public health emergency, prompted by growing concern that it could cause birth defects. As many as four million people could be infected by the end of the year. Officials at the Centers for Disease Control and Prevention have urged pregnant women against travel to about two dozen countries, mostly in the Caribbean and Latin America, where the outbreak is growing.
The infection appears to be linked to the development of unusually small heads and brain damage in newborns. Some pregnant women who have been to these regions should be tested for the infection, the agency said. Here are some answers and advice about the outbreak.
1. What is the Zika virus?
A tropical infection new to the Western Hemisphere.
The Zika virus is a mosquito-transmitted infection related to dengue, yellow fever and West Nile virus. Although it was discovered in the Zika forest in Uganda in 1947 and is common in Africa and Asia, it did not begin spreading widely in the Western Hemisphere until last May, when an outbreak occurred in Brazil.
Until now, almost no one on this side of the world had been infected. Few of us have immune defenses against the virus, so it is spreading rapidly. Millions of people in tropical regions of the Americas may now have been infected.
Yet for most, the infection causes no symptoms and leads to no lasting harm. Scientific concern is focused on women who become infected while pregnant and those who develop a temporary form of paralysis after exposure to the Zika virus.
2. How is the virus spread?
Mosquitoes, but not every species.
Zika is spread by mosquitoes of the Aedes genus, which can breed in a pool of water as small as a bottle cap and usually bite during the day. The aggressive yellow fever mosquito, Aedes aegypti, has spread most Zika cases, but that mosquito is common in the United States only in Florida, along the Gulf Coast, and in Hawaii – although it has been found as far north as Washington, D.C., in hot weather.
The Asian tiger mosquito, Aedes albopictus, is also known to transmit the virus, but it is not clear how efficiently. That mosquito ranges as far north as New York and Chicago in summer.
Although the virus is normally spread by mosquitoes, there has been one report of possible spread through blood transfusion and one of possible spread through sex. The virus was found on one occasion in semen.
3. How might Zika cause brain damage in infants?
Experts aren’t certain how it happens, or even whether the virus is to blame.
The possibility that the Zika virus causes microcephaly – unusually small heads and damaged brains – emerged only in October, when doctors in northern Brazil noticed a surge in babies with the condition.
It may be that other factors, such as simultaneous infection with other viruses, are contributing to the rise; investigators may even find that Zika virus is not the main cause, although right now circumstantial evidence suggests that it is.
It is not known how common microcephaly has become in Brazil’s outbreak. About three million babies are born in Brazil each year. Normally, about 150 cases of microcephaly are reported, and Brazil says it is investigating nearly 4,000 cases. Yet reported cases usually increase when people are alerted to a potential health crisis.
4. What is microcephaly?
Babies with microcephaly have unusually small heads. In roughly 15 percent of cases, a small head is just a small head, and there is no effect on the infant, according to Dr. Constantine Stratakis, a pediatric geneticist and a scientific director at the National Institute of Child Health and Human Development.
But in the remainder of cases, the infant’s brain may not have developed properly during pregnancy or may have stopped growing in the first years of life. These children may experience a range of problems, like developmental delays, intellectual deficits or hearing loss.
The consequences can vary widely from child to child. Pinpointing an underlying cause helps clinicians to advise parents about their newborn’s prognosis.
Genetic abnormalities are a common cause. Microcephaly can also be triggered by infections of the fetus, including German measles (also known as rubella), toxoplasmosis (a disease caused by a parasite found in undercooked contaminated meat and cat feces) and cytomegalovirus.
Microcephaly may also result if a pregnant woman consumes alcohol, is severely malnourished or has diabetes. If the defect occurs in a child’s first years, it may be a result of a brain injury during labor.
There is no treatment for an unusually small head.
“There is no way to fix the problem, just therapies to deal with the downstream consequences,” said Dr. Hannah M. Tully, a neurologist at Seattle Children’s Hospital who specializes in brain malformations.
5. What countries should pregnant women avoid?
About two dozen destinations mostly in the Caribbean, Central America and South America.
The Pan American Health Organization believes that the virus will spread locally in every country in the Americas except Canada and Chile. Here is the C.D.C.’s current list of countries and territories in which Zika virus is circulating. The latest updates are here.
6. How do I know if I’ve been infected? Is there a test?
It’s often a silent infection, and hard to diagnose.
Until recently, Zika was not considered a major threat because its symptoms are relatively mild. Only one of five people infected with the virus develop symptoms, which can include fever, rash, joint pain and red eyes. Those infected usually do not have to be hospitalized.
There is no widely available test for Zika infection. Because it is closely related to dengue and yellow fever, it may cross-react with antibody tests for those viruses. To detect Zika, a blood or tissue sample from the first week in the infection must be sent to an advanced laboratory so the virus can be detected through sophisticated molecular testing.
7. I’m pregnant and I recently visited a country with Zika virus. What do I do?
Some women should get blood tests, and just about all should get ultrasound scans.
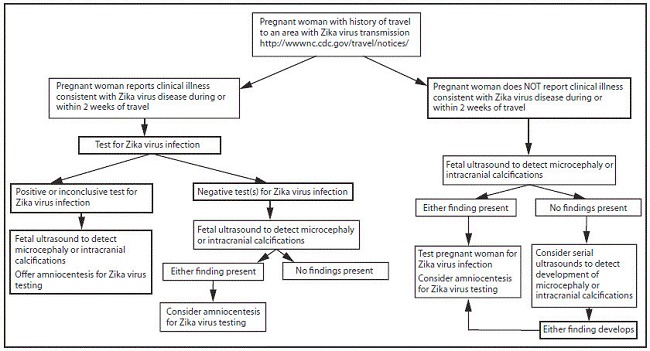
On Jan. 19, the C.D.C. issued interim guidelines for women in that situation and for their doctors. The guidelines are complex — and may change.
In general, they say that pregnant women who have visited any area with Zika transmission should consult a doctor. Those who have had symptoms of infection like fever, rash, joint pain and bloodshot eyes during their trip or within two weeks of returning should have a blood test for the virus.
That recommendation is controversial, because even women with no symptoms may have been infected — 80 percent of those who get the virus do not feel ill — and there is no evidence that babies are hurt only when the mother has been visibly ill. But at the time the guidelines were issued, the C.D.C. and state health departments simply did not have the laboratory capacity to test every pregnant woman who visited Latin America and the Caribbean in the last nine months, as well as every pregnant woman in Puerto Rico.
Even for women who get blood tests, the news is not entirely reassuring. Tests for the virus itself only work in the first week or so after infection. Tests for antibodies can be done later, but they may yield false positives if the woman has had dengue, yellow fever or even a yellow fever vaccine.
Under the C.D.C’s testing algorithm, pregnant women who have been to affected regions – whether they have symptoms or not, and whether they have negative or positive blood tests – should eventually have an ultrasound scan to see if their fetuses are developing microcephaly or calcification of the skull.
Unfortunately, an ultrasound usually cannot detect microcephaly before the end of the second trimester.
Some women also should have amniocentesis to test the fluid around the fetus for Zika virus. But amniocentesis involves piercing the amniotic sac with a long needle through the abdomen; it is slightly risky for the fetus and is not recommended before 15 weeks gestation.
Several companies are working on rapid tests for Zika infection. The C.D.C. also usually distributes test kits and training materials to state health departments during outbreaks, which should increase testing capacity.
8. I’m of childbearing age, but not pregnant and not planning to get pregnant. Should I go to an affected country?
Only if you use birth control religiously.
Half of pregnancies are unintended. If you want to visit a country where Zika transmission has been reported, Dr. Laura E. Riley, a specialist who works with high-risk pregnancies and infectious disease at Massachusetts General Hospital, advises strict use of birth control to ensure you don’t get pregnant.
Women who become unexpectedly pregnant while traveling or shortly afterward will face blood tests, monthly ultrasounds and a great deal of anxiety.
“Why would you ever sign yourself up for that?” said Dr. Riley. “There’s enough in life to worry about. I wouldn’t add that to my list.”
9. I’m pregnant now, but wasn’t when I visited one of the affected countries. What’s the risk?
Very low, experts say.
With rare exceptions, the virus does not appear to linger in the body, and people who recover from the infection are immune.
“Our understanding, thus far, is that the risk is very, very low if you were in that place prior to conception,” said Dr. Laura E. Riley of Massachusetts General Hospital.
“I wouldn’t be worried about if you conceived after you got back to the U.S.”
10. Does it matter when in her pregnancy a woman is infected with Zika virus?
Earlier in pregnancy seems to be more dangerous.
The most dangerous time is thought to be during the first trimester – when some women do not realize they are pregnant. Experts do not know how the virus enters the placenta and damages the growing brain of the fetus.
Closely related viruses, including yellow fever, dengue and West Nile, do not normally do so. Viruses from other families, including rubella (German measles) and cytomegalovirus, sometimes do.
11. Should infants be tested?
Other birth defects may be linked to the virus.
Federal health officials say that newborns should be tested for infection with the Zika virus if their mothers have visited or lived in any country experiencing an outbreak and if the mothers’ own tests are positive or inconclusive.
The reason, officials said in interviews, is that infection with the virus could be linked to defects in vision and hearing, among other abnormalities, even if the child does not suffer microcephaly. The other defects may require further assessments and testing.
The new guidance applies only to infants of mothers who reported symptoms of Zika virus infection — a rash, joint pain, red eyes or fever — while living abroad in an affected country or within two weeks of travel to such a destination.
12. Is there a treatment?
No.
The C.D.C. does not recommend a particular antiviral medication for people infected with the Zika virus. The symptoms are mild – when they appear at all – and usually require only rest, nourishment and other supportive care.
13. Is there a vaccine? How should people protect themselves?
Protection is difficult in mosquito-infested regions.
There is no vaccine against the Zika virus. Efforts to make one have just begun, and creating and testing a vaccine normally takes years and costs hundreds of millions of dollars.
Because it is impossible to completely prevent mosquito bites, the C.D.C. has advised pregnant women to avoid going to regions where Zika is being transmitted, and has advised women thinking of becoming pregnant to consult doctors before going.
Travelers to these countries are advised to avoid or minimize mosquito bites by staying in screened or air-conditioned rooms or sleeping under mosquito nets, wearing insect repellent at all times and wearing long pants, long sleeves, shoes and hats.
14. If Zika virus has been in Africa and Asia for decades, why wasn’t a link to microcephaly detected earlier?
It may be that the virus never had struck such a large population without immunity.
Microcephaly is rare, and it has many other causes, including infection of the fetus with rubella (German measles), cytomegalovirus or toxoplasmosis; poisoning of the fetus by alcohol, mercury or radiation; or severe maternal malnutrition and diabetes. It is also caused by several gene mutations, including Down syndrome.
Until recently, health officials paid little attention to Zika virus. It circulated in the same regions as dengue and chikungunya, and compared to those two painful infections – nicknamed “break-bone fever” and “bending-up fever” – Zika was usually mild.
The virus is thought to have reached Asia from Africa at least 50 years ago. While it may have caused spikes in microcephaly as it first spread, there was no testing to pin down which of many possible causes was to blame.
In 2007, a Southeast Asian strain of the Zika virus began leap-frogging the South Pacific, sparking rapid outbreaks on islands where no one had immunity to it. Because island populations are small, rare side effects did not occur often enough to be noticed. But in 2013, during an outbreak in French Polynesia, which has 270,000 residents, doctors confirmed 42 cases of Guillain-Barrê syndrome, which can cause paralysis. That was about eight times the normal number and the first hint that Zika virus can attack the nervous system, which includes the brain.
Zika was first confirmed in Brazil – a country of 200 million – last May, and it spread like wildfire. The first alarms about microcephaly were raised only in October, when doctors in the northeastern state of Pernambuco reported a surge in babies born with it. Pernambuco has nine million people and 129,000 annual births. In a typical year, nine are microcephalic infants.
By November 2015, when Brazil declared a health emergency, Pernambuco had had 646 such births.
15. Outside of Brazil has a Zika outbreak ever been linked to microcephaly?
Officials in French Polynesia have suspicions about an outbreak two years ago.
French Polynesia is the only area outside of Brazil to be affected by a Zika outbreak in which public health officials have identified an increase in the number of fetuses and babies with unusually small heads. There is “very high suspicion” of a link between the Zika virus and microcephaly in French Polynesia, said Dr. Didier Musso, an infectious disease specialist at the archipelago’s Institut Louis Malardé – though he said additional research was still needed.
Last November French Polynesian officials reinvestigated an outbreak of Zika that lasted from October 2013 to April 2014. They reported finding an unusual increase – from around one case annually to 17 cases in 2014-15 – of unborn babies developing “central nervous system malformations,” a classification that includes microcephaly.
There were no investigations at the time to determine whether the mothers were infected with Zika virus during pregnancy. Four of the mothers were tested later and the results indicated they may have been infected with the virus. Additional research is underway, Dr. Musso said.
Source: nytimes
RECTANGE HERE